
Why Do Shunts Fail? A Glimpse Into Shunt Valve Evolution
Introduction
Hydrocephalus affects many types of individuals, and ventriculoperitoneal (VP) shunts are still the most common treatment method. Even with all of the progress and new ideas over the years, shunt failure still remains a major issue in the hydrocephalus community. An estimated 30-50% of shunts fail within 2 years, with valve failure accounting for approximately 15% of revision surgeries. A recent review published in World Neurosurgery examined the evolution of shunt valves, how they have improved over time, and challenges that still arise. Here’s what you need to know:
Brief History
Early attempts to relieve pressure buildup involved mechanisms like skull punctures and external drains that often resulted in infection or overdrainage. Then in the 1960s, subcutaneous reservoirs – surgically implanted devices that can access body cavities or blood vessels for drainage – allowed doctors to remove cerebrospinal fluid (CSF) manually which seemed ideal but still presented many challenges. They required frequent tapping and had a high risk of infection.
A breakthrough emerged when valves were added to shunt systems because they allowed for more control over CSF drainage with a reduced risk of infection.
The Evolution of Shunt Valves
*Correction to the video: Anti-siphon devices and gravitation valves were first introduced in the 1970s-1980s.
First-Generation Valves
The first valves were created in the 1950s and 60s. They were very simple and acted as gatekeepers of CSF. When pressure in the brain reaches a specific, predetermined value, the valve opens to release fluid — and closes again when the pressure drops. These valves have fixed differential pressure, meaning the pressure required for the valve to open and release CSF cannot be adjusted. Some examples of first-generation valves include:
- Silt valves: CSF drained through slits in the silicone tubing; prone to wear and degradation over time.
 (doi.org/10.3390/jcm10061210)
(doi.org/10.3390/jcm10061210)
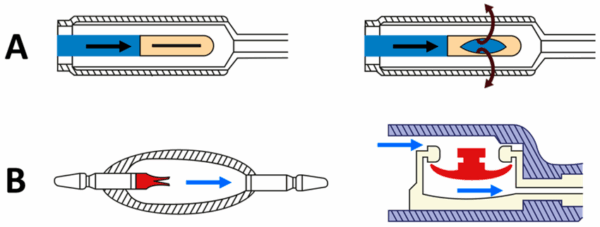
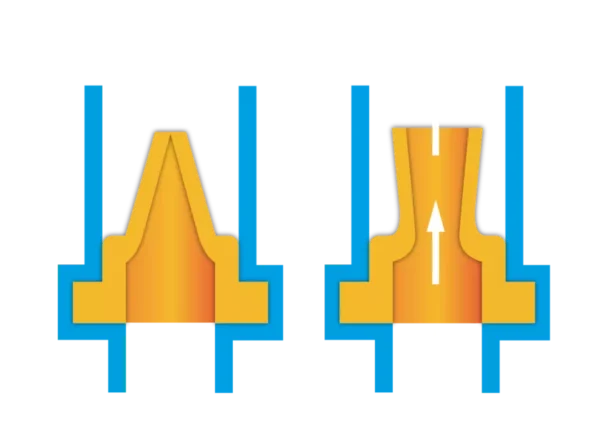
- Miter (duckbill) valves: CSF drained through simple flaps that opened with pressure; degraded quickly.
 (https://minivalve.com/valve-school/duckbill-valves-how-they-work/)
(https://minivalve.com/valve-school/duckbill-valves-how-they-work/)
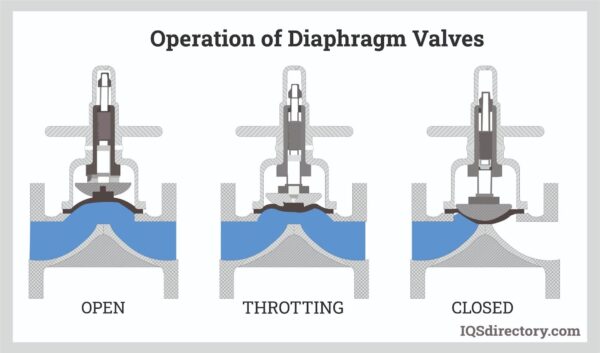
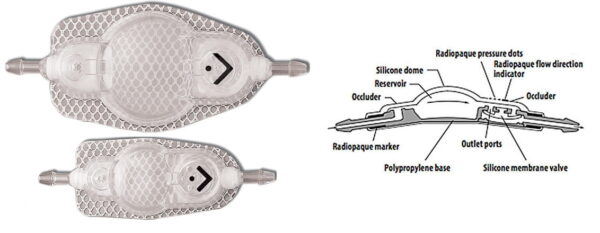
- Diaphragm valves: CSF drained through flexible membranes that cracked or wore out with repeated use.
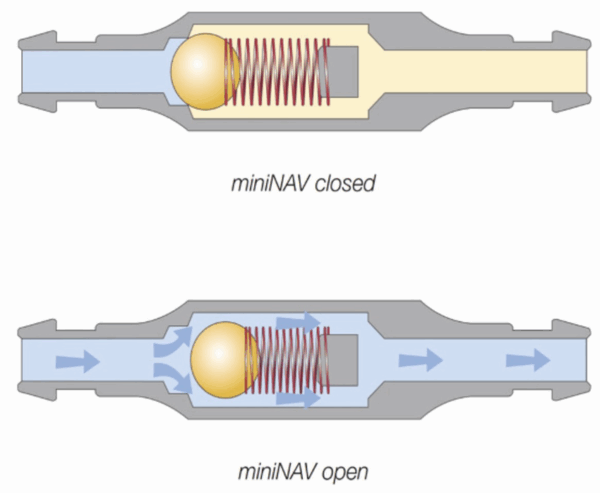
- Ball-in-cone valves: CSF drained through springs and balls that opened under pressure; much more reliable and still a foundation for modern valves.
 (doi.org/10.3389/fvets.2024.1435982)
(doi.org/10.3389/fvets.2024.1435982)
The main challenges that arose in first-generation valves included problems like hysteresis (delayed response), overdrainage with everyday movements–something as simple as sitting up, as well as no way to adjust settings after a surgery.
Second- and Third-Generation Valves
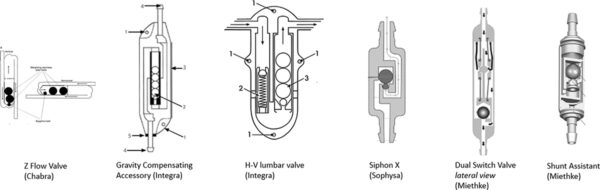
- Anti-siphon devices: First introduced in the 1970s, these were designed to fix the issue of overdrainage when standing up or performing other basic activities.
 (https://mriquestions.com/shuntsdrains.html)
(https://mriquestions.com/shuntsdrains.html)
- Gravitational valves: Developed in the 1980s and 90s, they utilized tiny weighted balls that shifted with body position, and helped prevent overdrainage from simple movements like standing up.
 (doi.org/10.1080/17434440.2020.1837622)
(doi.org/10.1080/17434440.2020.1837622)
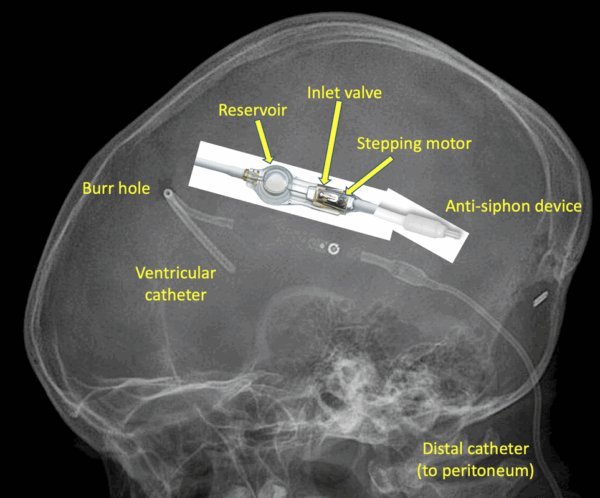
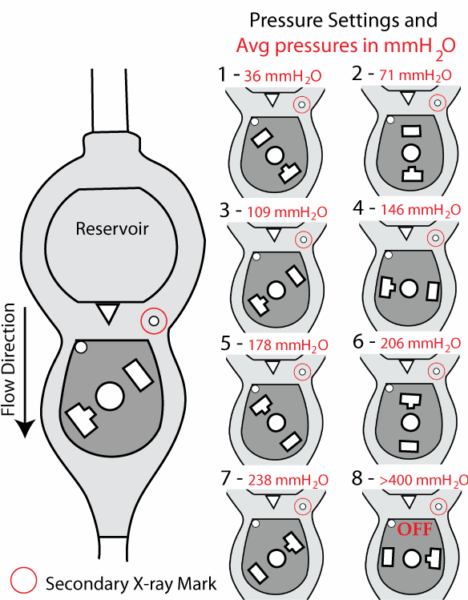
- Programmable valves: Emerging in the 1980s, these allowed doctors to adjust the valve’s opening pressure non-invasively (typically using a magnetic device). Unlike the fixed settings of first-generation valves, this meant patients didn’t need another surgery every time adjustments were required.
 (https://www.bocaradiology.com/shunt.html)
(https://www.bocaradiology.com/shunt.html)
- Flow-reducing devices: Created in the late 20th century, these devices smooth out sudden pressure spikes from actions like sneezing, coughing, or standing up, which first-generation valves didn’t have the power to do.
 (Medtronic)
(Medtronic)
These innovations make valves more flexible and safe, but also more complicated.
Why Valves Still Fail:
- Wear and tear of material, like silicone and springs, that cause structural issues to the valve, potentially resulting in underdrainage or overdrainage.
- Blockages due to cell and protein buildup inside the valve.
- Magnetic fields from MRI’s or other environments that cause valve settings to change (especially common in older programmable valves).
- Handling damage during surgery or trauma after implantation.
- Difficulty in picking the right valve and setting for each person because hydrocephalus cases are incredibly unique.
Patient-Specific Challenges
It can be very difficult to find the “perfect” valve for a hydrocephalus patient because there are many factors that affect its functionality. The right valve depends on age, condition, CSF production and flow rates, and even skull shape.
Looking Ahead
Researchers are currently exploring new ideas:
- Focused ultrasound to non-invasively clear tissue and debris from valves to avoid shunt blockages (check out our Emerging Tech: Focused Ultrasounds blog here).
- Cranial implants to hide the common valve bump and reduce scalp breakdown (e.g., InvisiShunt® by Longeviti).
- More durable material and better designs that are less prone to failure.
- Smart shunts that monitor pressure continuously and adjust drainage automatically (check out our Emerging Tech: Smart Shunts blog here).
- Flushing devices to clear catheter holes to restore, increase, or maintain flow (e.g., ReFlow™ by Anuncia Medical).
- Minimally invasive treatments to avoid the need for traditional brain surgery (e.g., eShunt® System by CereVasc).
Even though shunt valves have come a long way, the perfect solution is still not here – yet. Nonetheless, it is critical to understand how shunt valves work and why they can fail to help patients and families make informed decisions and advocate for themselves. Continued research is coming closer to improved valves that will last much longer, respond better, and work more reliably for people living with hydrocephalus.